

Addressing Problems In Total Shoulder Replacement Surgery
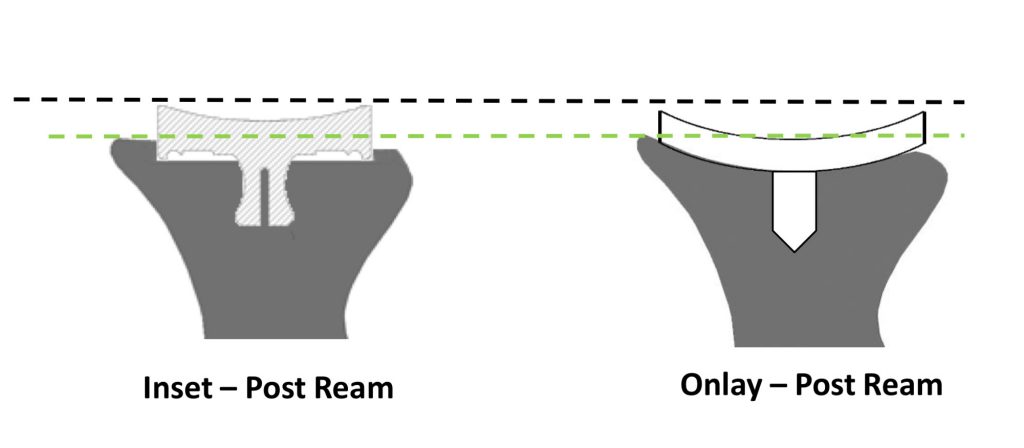
The problems encountered with current total shoulder replacement models are based upon the fact that the glenoid sits on top of the bony surface.
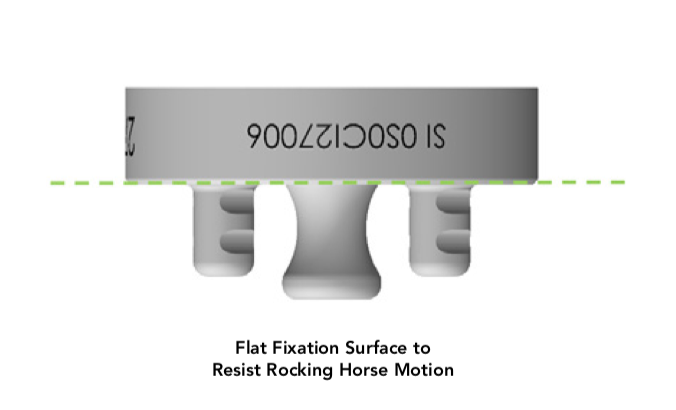
So when the humerus goes up and down, rotates, and slides back-and-forth, it rocks the glenoid loose potentially because it’s sitting on the surface.
InSet™ Glenoid
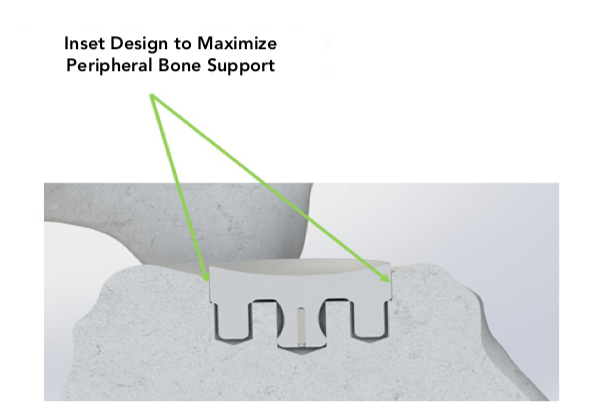
This problem is solved with an InSet™ glenoid because the glenoid doesn’t sit on the surface. The implant sits partially within the bone like a manhole cover surrounded by a peripheral rim of strong sclerotic bone.
Another advantage of this InSet™ glenoid fixation is that because there’s such a strong circumferential rim of cortical bone, you don’t need much backside fixation and you can place the implant in deficient bone without much bony support.
New scientific data presented in the literature in the Journal of Shoulder and Elbow Surgery shows that the InSet™ glenoid fixation technique increases the strength of fixation by up to 40 times.
Our InSet™ glenoid technology significantly reduces surgical exposure and, in FEA models, improves glenoid stability by 87%.
InSet™ Glenoid Technique
This InSet™ Glenoid Technique Video from Peter S. Johnston, MD demonstrates the approach to the glenoid in total shoulder arthroplasty with the use of an InSet™ Glenoid component.
15 Day Post Op Video
61- year old right-hand dominant man with more than 5 years of progressive shoulder discomfort who sought Dr. Adkison for a second opinion after failing all conservative measures.
Preoperative range of motion was 100 degrees of elevation, 30 degrees external rotation at the side, 70 degrees abduction, and internal rotation to the mid-lateral iliac crest.
He had not been able to thread his belt for about 15 years.
He underwent TSA through the rotator interval approach using an InSet™ glenoid as an outpatient.
His first follow up at 15 days is recorded on the video.